
Colorectal tumor has a major impact on global health and, according to INCA data, it ranked second in incidence in both sexes in our country in 2020. Complications resulting from colorectal tumor rank second in cancer mortality worldwide6. At diagnosis, about 20% of these patients already present with hepatic metastases.4
With the advancement of oncological treatments and better understanding of the disease, a greater number of treatments are available for these patients, including: surgery, chemotherapy, immunotherapy, radiotherapy and radio interventional treatments. Although patients with hepatic metastases are considered stage IV, they are still cases eligible for curative treatment.
Faced with several therapeutic options and with the increase in survival, complex cases have become more common, which requires us to have a deep knowledge of the different therapeutic options. Recognizing this difficulty, oncology hospitals organize specialized multidisciplinary committees that discuss the particularities of each patient with the intention of obtaining the best results. It is in these meetings that we outline the therapeutic planning and the best time for reassessment and action of each team.

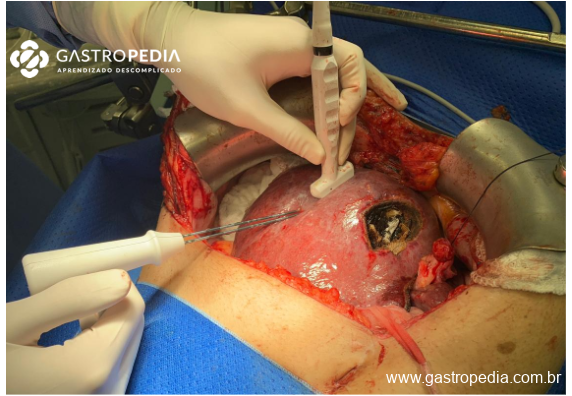
Figure 1 – Performing radiofrequency ablation guided by simultaneous ultrasound to hepatic surgery for multimodal treatment of colorectal tumor metastases
Given the epidemiological importance of the diagnosis that frequently presents in clinics and in emergency situations – where we do not always have access to multidisciplinary opinion in a timely manner – this article aims to show the benefits and disadvantages of each available strategy to offer to the patient with colorectal tumor and synchronous hepatic metastasis.
The studies on hepatic metastases from colorectal tumors are numerous and there is often a regional difference in terminology on the subject. This article applies to patients with hepatic metastasis already existing or identified at the staging of the primary tumor.

Figure 2 – Magnetic resonance imaging showing synchronous hepatic metastasis (yellow arrow) to a right colon adenocarcinoma (blue arrow).
Patients with asymptomatic colorectal tumor and resectable hepatic metastases
Most clinical and surgical specialists recommend preoperative chemotherapy – for about 02 months – followed by surgical treatment if good response1. Surgery can involve resection of the primary in association with hepatectomy as long as the surgeons are qualified for this and that both are medium-sized surgeries. Casuistics have already shown a higher rate of perioperative complications and mortality in cases of combined surgery involving major hepatectomies2.
It is also possible to perform resection of the primary followed by chemotherapy in the interval between surgeries; with hepatic resection scheduled for after about 2 to 3 months. During the first surgery, the evaluation of hepatic disease and histopathological confirmation of metastases can be performed, if necessary.

Figure 3 – Intraoperative laparoscopic ultrasound. Valid resource in the identification and intraoperative planning of hepatic resections.
There was no difference in survival over a 5-year period when analyzing the options; however, we highlight that these are data from retrospective studies in which there may have been a bias in the indication of primary surgery for patients with better performance and less volume of oncological disease. Therefore, the consensus among specialized centers is to indicate chemotherapy as the first treatment1.
Patients with asymptomatic colorectal tumor and unresectable hepatic metastases
It is common for cases of colorectal tumors in patients with good performance to undergo surgery as the first treatment regardless of the presence of hepatic metastases. However, it is observed that the limiting factor for the possible curative treatment of these patients is the systemic disease manifested in the liver3.
Therefore, it is recommended to perform chemotherapy as the first treatment, with reassessment of the response after 2 months and programming of the hepatectomy, if feasible. In 1996, Bismuth already demonstrated a conversion rate of unresectable hepatic metastases to resectable in 16% with impact on prognosis (survival rate of 40% in 05 years). More recent results show conversion rates of up to 30%2.
The literature shows that the outcome of patients who, in the end, underwent both surgeries is similar whether for those who started treatment with chemotherapy, or for those who started with colectomy. This data gives us confidence to keep the primary lesion under treatment with chemotherapy and, at the same time, pursue the possibility of surgical treatment – simultaneous or in stages – of all lesions1.

Figure 4 – In addition to the reduction in dimensions after chemotherapy, there is a change in signal (scar aspect) and better delimitation of the lesion limits; factors that favor the surgical procedure
Patients with symptomatic colorectal tumor and hepatic metastases
It is estimated that about 20% of colorectal tumor cases have their diagnosis and treatment started in an emergency.5 In this context, it is important to highlight the impact of complete staging in the face of clinical suspicion of colorectal tumor. If it is safe for the patient, performing contrast-enhanced abdominal and thoracic tomography and carcinoembryonic antigen dosage before a possible resection of the primary tumor will be fundamental during oncological therapeutic planning.
The main complications that lead the patient with colorectal tumor to emergency are intestinal obstruction, perforation or bleeding. Even in the face of a metastatic patient, we need to consider the patient as potentially treatable and, therefore, offer a surgery with oncological principles or a derivation that allows to delay the treatment with curative intentions1.
There is consensus among specialists that during the symptomatic context with obstruction or perforation there is no room to involve any approach to hepatic metastases.1
Bleeding in colorectal tumor rarely requires emergency surgery. In general, bleeding can be solved with transfusion therapy followed by early chemotherapy with good response. Once the bleeding is resolved, these patients can be managed according to the strategies above.
The different surgical treatment strategies
- Traditional
The strategy of the traditional approach consists in performing colectomy as the first treatment, followed by chemotherapy and hepatic surgery in 2-3 months2. On the one hand, this path is safer with the reduction of the risk of complications of the primary tumor. On the other hand, it is important to pay attention to the risk of complication during the resection of the primary that can, and often exceeds, the risk of intercurrences if we keep it under chemotherapy treatment.
A perioperative complication will delay the treatment of the patient’s systemic metastases, which is what will actually define his prognosis. Therefore, in cases of unresectable hepatic lesion, strongly consider starting with chemotherapy that may provide the opportunity for a complete treatment1.
- Simultaneous surgery
There are clear benefits to offering a combined treatment during just one surgical act. Being subjected to a single anesthetic act and a shorter hospital stay is an inviting possibility for the surgeon and the patient. However, prolonged operative time and a higher risk of perioperative complications are disadvantages already demonstrated and that, when they occur, nullify these benefits.
Currently, combined resection is reserved for cases of simple colectomy and minor hepatectomies that can be performed at the same surgical time by conventional or videolaparoscopic approach. The right subcostal incision of the hepatectomy allows the performance of oncological right colectomy, being this the most frequent indication. For cases of left colectomy, the laparoscopic approach with resection of smaller and peripheral nodules is the most used.
Increased mortality and morbidity have already been demonstrated in the association of large oncological colectomies (mesorectum approach or multivisceral) and/or major hepatectomies (resection of more than 3 segments); suggesting the limits of this type of strategy.5

Figure 5 – The simultaneous approach of primary tumor (right colon) and hepatic metastasis.
- Liver-first or Reverse Approach
Approach is increasingly used and reserved for cases where the complete oncological treatment will depend on a major hepatectomy and/or response of the lesions to chemotherapy.
Very applied in cases of medium/low rectal tumors where neoadjuvant chemotherapy and radiotherapy will be performed. In this interval, it is possible to start the treatment of hepatic disease over the time of response of the primary to chemoradiotherapy1.
The disadvantage of this strategy is the attention and monitoring of the symptoms of the primary tumor or its complications, such as intestinal obstruction and perforation. Studies show that the incidence of these local complications in asymptomatic patients during chemotherapy is low, but not null.7
References
- Adam, R. et al. Managing synchronous liver metastases from colorectal cancer: A multidisciplinary international consensus. 41, 729–741 (2022).
- Lillemoe, H. A. & Vauthey, J. Surgical approach to synchronous colorectal liver metastases: staged, combined, or reverse strategy. 9, 25–34 (2020).
- Siriwardena, A. K., Mason, J. M., Mullamitha, S. & Hancock, H. C. Management of colorectal cancer presenting with synchronous liver metastases. Nat. Publ. Gr. 11, 446–459 (2014).Borner MM. Neoadjuvant chemotherapy for unresectable liver metastases of colorectal cancer–too good to be true?. Ann Oncol. 10(6):623-626. (1999)
- Reddy SK, Pawlik TM, Zorzi D, et al. Simultaneous resections of colorectal cancer and synchronous liver metastases: A multi-institutional analysis. Ann Surg Oncol. 14:3481-91 (2007)
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 71(3):209-249. (2021)
- Tebbutt NC, Norman AR, Cunningham D, et al. Intestinal complications after chemotherapy for patients with unresected primary colorectal cancer and synchronous metastases. Gut. 52(4):568-573 (2003)
How to cite this article
Magalhães DP. Synchronous colorectal hepatic metastasis – How to program the treatment
Residência médica em Cirurgia Geral e Cirurgia do Aparelho Digestivo pelo Hospital das Clínicas da FMUSP.
Cirurgião voluntário do Serviço de Pâncreas e Vias Biliares do Hospital das Clínicas - USP.
Cirurgião do Aparelho Digestivo no Hospital Israelita Albert Einstein

{kind=link}