
Treating and caring for an oncology patient should go beyond the knowledge of high complexity and evidence-based that is updated every day. A solid doctor-patient relationship with expectation management and a lot of trust is expected.
The situation I want to put here is that of a patient with cholestatic syndrome due to non-biopsied periampullary malignant neoplasia. He had a very good status, a totally independent athlete for daily activities and with little weight loss even in the presence of symptoms of food intolerance.
Not meeting criteria for neoadjuvant (borderline)1 and without evidence of metastatic lesions in the staging performed, a resection was chosen as the first treatment (upfront) which took place about 1 month after the first contact with the surgeon.
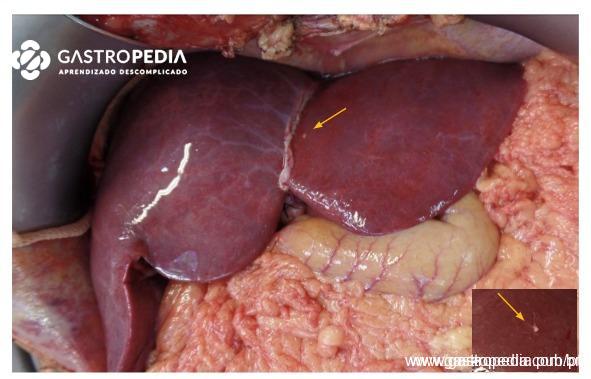
I expose the intraoperative photo:

The subcentimetric lesion highlighted was resected and sent for freezing biopsy. The finding was malignant neoplasia in the sample sent.
There are several factors at this decision-making moment that induce us to proceed with the surgery: the fallibility of intraoperative freezing, the fact that this patient – the exception of most cases attended in this context – is so physically and nutritionally fit for surgery, the confidence and optimism transmitted in consultation to the patient and family in the face of the precocity of surgical treatment, the experience of previous cases that were “successful”.
For this reason, I share the following studies that aimed to define the real prognosis of this patient.
What do the studies say?
In the first2 patients undergoing pancreatectomies associated with hepatic resections at an internationally renowned center were retrospectively analyzed.
The sample size (22 patients) is criticizable and is probably a consequence of high patient selection. This selection is also proven in the sample details: average size of the metastasis (0.6 cm), hepatic resections were mostly nodulectomies. In addition, all cases were similar to ours, an incidental intraoperative finding.
For control, two groups were designated: 1 – conventional resection with the same primary site without association with hepatic metastasis and 2 – palliative surgery performed in the face of hepatic metastasis (bili-digestive + food diversion). The comparison showed interesting but not unexpected results: at a cost of a higher rate of complications, bleeding and length of stay, there was no benefit in the survival of these patients in the long term compared to palliative surgery. It is worth noting that, as in our situation, we are comparing a group selected by optimism, by the expectation of better evolution compared to the usual.
I also highlight this more recent systematic review3 showing a similar survival between patients who underwent combined surgery in the proposed context and patients referred for palliative chemotherapy after metastasis detection in staging (not submitted to surgery). In selected patients, after chemotherapy and systemic control, the survival provided by the same surgery was 3 to 4 times greater.
Conclusion
As seen above, we are not lacking examples that in a few patients the surgery initially thought (resection of hepatic metastasis + duodenopancreatectomy) can bring benefit in survival4. However, at the time of surgery this individual has not yet gone through this selection of systemic treatment and, therefore, we do not yet know if he is – or better – will be one of these cases. Therefore, on that day, we proceeded with the bili-digestive diversion – thus solving the biliary obstruction – associated with food diversion due to the food symptoms alleged.
For those who would choose to proceed with the procedure, I invite you to reflect: no matter how optimistic our expectation, our intention and attitude remain subject to data and statistics. Our main function during our patient’s journey is to advise him to take the most advantageous path and not just hope for the best result.
After all, there are less risky surgeries that relieve symptoms and provide a systemic treatment without complications for our patient. In this way, in the light of current knowledge, he will remain with a higher quality of life and for a longer time outside the hospital environment. Remembering that definitive treatment will not cease to be an option if it proves adequate over its evolution.
Learn more about hepatic metastases. Click here
References
- Isaji, S. et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 18, 2–11 (2018).
- Gleisner, A. L. et al. Is resection of periampullary or pancreatic adenocarcinoma with synchronous hepatic metastasis justified? Cancer 110, 2484–2492 (2007).
- Crippa, S. et al. A systematic review of surgical resection of liver-only synchronous metastases from pancreatic cancer in the era of multiagent chemotherapy. Updates Surg. 72, 39–45 (2020).
- Nagai, M. et al. Oncologic resection of pancreatic cancer with isolated liver metastasis: Favorable outcomes in select patients. J. Hepatobiliary. Pancreat. Sci. 1–11 (2023) doi:10.1002/jhbp.1303.
How to cite this article
Magalhães DP. Periampullary neoplasia with isolated hepatic metastasis: what would you do? Gastropedia, vol. 2 Available at: gastropedia.com.br/cirurgia/neoplasia-periampular-com-metastase-hepatica-isolada-o-que-voce-faria/
Residência médica em Cirurgia Geral e Cirurgia do Aparelho Digestivo pelo Hospital das Clínicas da FMUSP.
Cirurgião voluntário do Serviço de Pâncreas e Vias Biliares do Hospital das Clínicas - USP.
Cirurgião do Aparelho Digestivo no Hospital Israelita Albert Einstein

{kind=link}