
Insulinoma is the most frequent functioning pancreatic neuroendocrine tumor (55%), with its peak occurrence in patients in their fifth decade of life (between 40 and 50 years) and a slight predominance among women (1.4:1)1.
The symptoms associated with the tumor are divided between adrenergic – anxiety, tremors and agitation – and neuroglycopenic such as disorientation, visual alterations and seizures2. Due to frequent food intake to avoid severe hypoglycemia during fasting, it is common for patients to present with obesity/overweight at diagnosis.
In 1938, the Whipple triad was described: documented hypoglycemia (<50mg/dL), symptomatic and relieved after caloric intake. Currently, diagnostic confirmation is given with a clinical fasting test of 48 to 72 hours in which laboratory tests are collected periodically. The laboratory profile will show low blood sugar in opposition to high levels of insulin, pro-insulin and C-peptide3. It is essential for diagnosis to ensure that the patient does not use oral antidiabetics such as sulfonylureas or injectable insulin.
The relationship of insulinoma in endocrine syndromes (MEN-1 and tuberous sclerosis) is known and brings propaedeutic particularities due to a higher risk of multiple neuroendocrine tumors or malignant insulinomas4.

The recommended treatment is surgical excision of the tumor. Enucleation, as well as segmental pancreatectomies, are recognized treatments since the vast majority of tumors are benign. Thus, lymphadenectomy becomes less relevant than the preservation of pancreatic parenchyma in order to avoid exocrine or endocrine insufficiency1.
Therefore, this article aims to bring an analysis of the different diagnostic tests used in insulinoma cases and their applications, in addition to a list of specific perioperative care for these patients.
Diagnostic methods by image
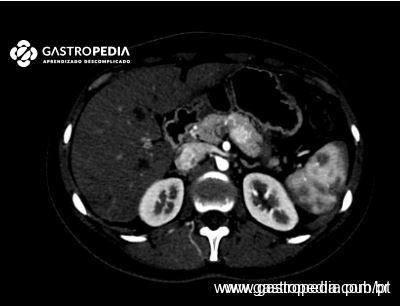
Axial methods with contrast are the most used for the anatomical study of the pancreas and its vascular relations. Among them, magnetic resonance, when available, has proven to be more sensitive to locate insulinomas that present as hypervascular nodules in the arterial phase, with hyperintensity in T2 and hypointensity in T1 in relation to the pancreatic parenchyma. Smaller lesions can be located more easily in diffusion phases5.


A specific exam for neuroendocrine tumors that uses their somatostatin receptors, the PET Gallium 68 can assist in cases of clinical suspicion without diagnosis by the methods above. It is an appropriate exam for the location of ectopic insulinomas that were not visualized in the upper abdomen5.
Invasive diagnostic methods
Echoendoscopy: Exam for evaluation of the pancreatic parenchyma in search of subcentimetric lesions, used by some authors as the first exam to locate the insulinoma. It offers even greater sensitivity in lesions of the head of the pancreas and uncinate process.
In the report of a suspected insulinoma, it is important to include, if possible, the measurement of the tumor, its location and the distance from relevant vascular structures (spleno-mesenteric junction), and the proximity of the main pancreatic duct (to assist the operative decision to enucleate the lesion).1

Needle puncture is dispensable in the vast majority of cases. The symptomatic patient with sporadic lesion does not need histopathological confirmation for treatment. In endocrine syndromes, both functioning and non-functioning neuroendocrine tumors can express immunohistochemical markers for insulin. Thus, this exam is not suitable to differentiate them. 6
In non-peripheral or intrapancreatic lesions of difficult location, the surgeon may request a tattoo with methylene blue to facilitate intraoperative location.
Selective pancreatic arterial catheterization (SACS)
The exam consists of positioning a collector catheter in the right hepatic vein to collect the blood level of insulin after arterial stimuli.
Then, after selective arterial catheterization, calcium gluconate is injected into the peripancreatic arteries with the power to topograph the lesion if insulinemia doubles within 3 minutes after injection.
- Tumor in the body/tail of the pancreas: Positive after injection in the splenic artery
- Tumor in the pancreatic head or uncinate process: Positive after injection in the gastroduodenal or superior mesenteric artery
- Hidden hepatic metastasis: Positive after injection in the proper hepatic artery

The exam is used mainly in cases of endocrine syndromes and multiple neuroendocrine tumors in which it is desired to identify which lesion is metabolically active.1
Surgical treatment
The definition of surgical route depends on the surgeon’s expertise. It is important to note that for laparoscopic access, especially for nodulectomies and distal pancreatectomies, a detailed planning of the location of the pancreatic section is necessary. Conversion to open surgery is justified in cases of imprecision.7

Intraoperative ultrasonography is an ally of the liver and pancreas surgeon and, in this context, certifies the tumor location and proximity to pancreatic ducts in cases where enucleation is considered. Thus, the exam provides greater safety to the procedure, reducing the risk of pancreatic fistula and allowing preservation of pancreatic parenchyma when possible.

Residência médica em Cirurgia Geral e Cirurgia do Aparelho Digestivo pelo Hospital das Clínicas da FMUSP.
Cirurgião voluntário do Serviço de Pâncreas e Vias Biliares do Hospital das Clínicas - USP.
Cirurgião do Aparelho Digestivo no Hospital Israelita Albert Einstein

{kind=link}