
Infection with H. pylori and the use of non-steroidal anti-inflammatory drugs (NSAIDs) are widely accepted as the main causes of peptic ulcer. However, with more effective eradication, better sanitary conditions and widespread use of antibiotics, the prevalence of H. pylori is falling and, consequently, there is an increase in the diagnosis of non-H. pylori ulcers.
The proportion of non-H. pylori and non-NSAID/aspirin ulcers varies quite a bit (from 2 to 35%) according to the time, country and methodology of different studies:
- A multicenter prospective French study published a decade ago included 713 patients and concluded that 1 in 5 ulcers was not related to either H. pylori or the use of NSAIDs/aspirin.
- A retrospective Brazilian study published in 2015 (De Carli, DM et al), in turn, identified that, from 1997 to 2000, 73.3% of peptic ulcers were due to positive H. pylori, 3.5% due to NSAIDs, 12.8% due to H. pylori + NSAIDs and 10.4% idiopathic, while, from 2007 to 2010, this proportion became, respectively, 46.4%, 13.3%, 19.9% and 20.5%.
But what would be the other possible etiologies for gastric and duodenal ulcers?
Table 1: Possible etiologies for gastric and duodenal ulcers not associated with Helicobacter pylori and the use of NSAID
| Etiology | Comment |
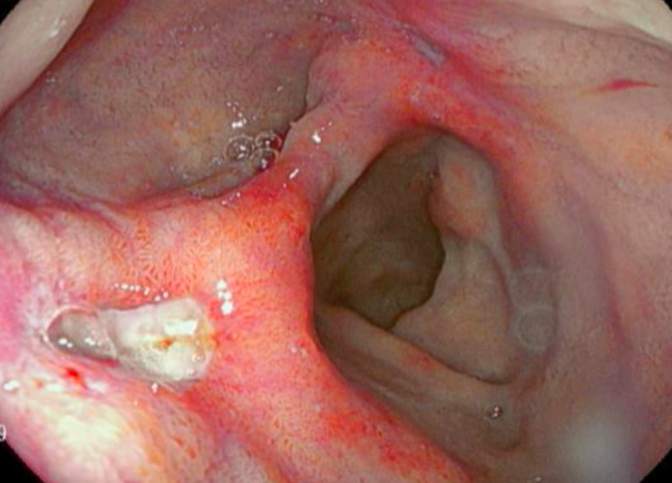
| Neoplasia (Adenocarcinoma, Lymphoma, GIST, Leiomyosarcoma) | The possibility of malignancy should always be considered in the case of gastric ulcers (including for this reason we should always biopsy gastric ulcers and always perform an examination to confirm their healing). Adenocarcinoma is the most prevalent (95% of cases). More suspicious characteristics are: necrotic background and raised and irregular edges. |
| Zollinger-Ellison Syndrome | Secondary to gastrinoma (single or multifocal, located in pancreas or small intestine). Patient presents with abdominal pain + diarrhea, with multiple ulcers usually refractory or recurrent. 25 to 30% of patients who develop gastrinoma have multiple endocrine neoplasia type 1 (MEN1 – multifocal primary hyperparathyroidism, pancreatic islet tumors and pituitary adenomas). |
| Non-NSAID medications (Bisphosphonates, Corticosteroids, Clopidogrel, selective serotonin reuptake inhibitors, potassium chloride) | The isolated association of these medications with ulcer disease is controversial, but they certainly have a synergistic action with the use of NSAIDs |
| Infections | – Duodenal colonization by H. pylori- Non-pylori Helicobacter: the most common is Helicobacter heilmannii- Virus (herpes simplex type I, Cytomegalovirus, EBV): the biopsy will be definitive for the diagnosis. – Syphilis- Tuberculosis |
| Systemic mastocytosis | Characterized by infiltration of mast cells in many tissues and symptoms of flushing, itching, tachycardia, abdominal pain and diarrhea. Dyspepsia, ulcers and duodenitis occur in 30 to 50% of cases. It is considered that the production of histamine by mast cells results in excessive stimulation of acid production. Serum tryptase may be increased. In the ulcer biopsy, infiltration of the mucosa by mast cells can be identified. |
| Ischemic (Arterial or venous disease / Vasculitis) | Ischemic ulcers can result from vascular insufficiency secondary to hypotension, vasculitis or thromboembolism. However, they are rare, as there is a rich collateral circulation in the region. Biopsies may suggest ischemia and, in case of suspicion, an abdominal angiotomography may assist. |
| Drug use | Cocaine, crack and amphetamines cause tissue ischemia by vasoconstriction |
| Post-surgical | After subtotal gastrectomy (anastomotic edge ulcer). The etiology can be multifactorial:- Local ischemia- Anastomotic tension- Retained gastric antrum syndrome: when a small portion of the antral mucosa containing G cells remains in the proximal portion of the duodenum. This gastric antrum mucosa at the end of the duodenal loop is then stimulated by the alkaline duodenal environment to continuously secrete gastrin. |
| Granulomatous diseases (Crohn, Sarcoidosis) | – Only 0.3% to 5% of cases of Crohn’s disease involve the upper gastrointestinal tract. – Gastrointestinal involvement is very rare in sarcoidosis, but when it occurs it mainly affects the stomach. Gastric sarcoidosis can present as an ulcer or as diffuse involvement (similar to plastic linitis). |
| Hyperparathyroidism | Calcium stimulates the release of gastrin, but the clinical relevance of this effect is not certain. |
| Eosinophilic gastroenteritis | It is a rare and heterogeneous clinical condition, which can involve any segment of the gastrointestinal tract. The pathogenesis is not yet well established, but there is an association with atopic conditions, such as asthma, rhinitis and eczema. Laboratory tests show peripheral blood eosinophilia in 70 to 80% of cases and increased serum IgE in up to two thirds of patients. The identification of dense infiltration of eosinophils in the biopsy is a major diagnostic marker. |
| Stress ulcer | Ulcer that occurs due to hospitalization, mainly in patients in the intensive care unit. |
| Chronic diseases (Cirrhosis, chronic kidney disease, diabetes) | These patients generally have lower H. pylori eradication success rates and lower PPI efficacy than those without chronic diseases |
| Radiotherapy | The stomach and duodenum are sometimes involved in the radiation field during the treatment of some tumors. Radiation-induced ulcers are difficult to treat and usually do not heal with conventional anti-acid secretory agents, surgical procedures may be necessary. |
| Idiopathic | – |
How to investigate, then, the etiology of the ulcer?
1. Confirm that there really is no H. pylori:
it is necessary to make sure that H. pylori was properly researched. It is considered that the main cause of negative H. pylori ulcer is actually the error in detecting the microorganism. We should check:
- Was the exam performed in the context of bleeding? If so, it is ideal to repeat. Hemorrhagic peptic ulcer can produce up to 25% false negative results in the urease test;
- Did the patient stop PPI and antibiotics before endoscopy? For practical purposes, diagnostic tests for H. pylori should be delayed for 4 weeks after the use of antibiotics, bismuth preparations, PPI and H2 blockers.
- What method used for research? If possible, it is interesting to perform at least two simultaneous tests to increase sensitivity. Histological research should include at least two biopsies of antrum and body.
2. Confirm that the patient really did not use NSAIDs:
Often, the patient forgets that they may have used or does not associate the class with the medication. It is important to actively ask for the medications (name them) and if they did not use treatments, for example, for headache, arthralgia, dental treatment or menstrual cramps. Chinese herbal medicines, compounded medications and alternative therapy products may contain anti-inflammatory compounds, which are not recognized by patients. Also check for the use of ASA, even at low doses.
If we really do not confirm that H. pylori was negative and that there is no report of NSAIDs, we should reinforce some important points in the clinical history:
- Use of other medications;
- Use of drugs;
- History of immunosuppression;
- History of gastric surgeries or radiation;
- History of comorbidities, such as Crohn’s Disease, sarcoidosis, systemic mastocytosis, MEN 1 (multifocal primary hyperparathyroidism, pancreatic islet tumors and pituitary adenomas)
- Associated symptoms, mainly diarrhea (which can be associated with Crohn’s Disease, Zollinger-Ellison Syndrome or systemic mastocytosis);
- Family history of ulcer or MEN 1.
3. Ulcer biopsy
Although often unspecific, the biopsy of the ulcer (especially gastric) is fundamental for the investigation of less usual etiologies. Immunohistochemical analysis can bring important additional information.
Additional complementary exams should be performed according to clinical suspicion, such as:
– Serum gastrin: If suspicion of Zollinger-Ellison;
– PTH and calcium: Investigation of hyperparathyroidism;
– VDRL: If suspicion of infectious ulcer;
– Serum tryptase: Can assist in the suspicion of systemic mastocytosis.
In patients with an ulcer without a well-established etiology, it is recommended to repeat endoscopy 8 to 12 weeks after treatment, with new biopsies if the ulcer is still present. It may also be interesting to biopsy the duodenum to detect isolated duodenal colonization of HP.
Conclusion
False negative test for H. pylori and failure to detect NSAID use are probably the most common causes of ulcers that apparently have no defined etiology. Once these possibilities are excluded, we should focus on a detailed anamnesis and a careful evaluation of the anatomopathological.
References
- Chung CS, Chiang TH, Lee YC. A systematic approach for the diagnosis and treatment of idiopathic peptic ulcers. Korean J Intern Med 2015;30:559–70. doi:10.3904/kjim.2015.30.5.559.
- Kim HU. Diagnostic and treatment approaches for refractory peptic ulcers. Clin Endosc 2015;48:285–90. doi:10.5946/ce.2015.48.4.285.
- Charpignon C, Lesgourgues B, Pariente A, Nahon S, Pelaquier A, Gatineau-Sailliant G, et al. Peptic ulcer disease: One in five is related to neither Helicobacter pylori nor aspirin/NSAID intake. Aliment Pharmacol Ther 2013;38:946–54. doi:10.1111/apt.12465.
- de Carli DM, Pires RC, Rohde SL, Kavalco CM, Fagundes RB. Different frequencies of peptic ulcer related to H. pylori or NSAIDs. Arq Gastroenterol 2015;52:46–9. doi:10.1590/S0004-28032015000100010.
- Lanas A, Chan FKL. Peptic ulcer disease. Lancet 2017;390:613–24. doi:10.1016/S0140-6736(16)32404-7.
How to cite this article
Lages RB. Ulcers not related to Helicobacter pylori and anti-inflammatory drugs (NSAIDs): how to proceed? Gastropedia 2023, Vol 1. Available at: https://gastropedia.com.br/gastroenterology/ulcers-not-related-to-helicobacter-pylori-and-anti-inflammatory-drugs-nsaids-how-to-proceed/
Médico do Departamento de Gastroenterologia do Hospital das Clínicas de São Paulo
Residência de Gastroenterologia e Endoscopia Digestiva pelo Hospital das Clínicas-FMUSP

{kind=link}